



Manufacturers are asking for more data than ever before. If your team is trying to figure out what to submit, to whom, and whether you are actually required to do it, you are not alone. These questions came up more than almost any other topic in our recent live Q&A, and for good reason. The landscape shifted significantly in the first half of 2026, and the decisions covered entities make now will have real financial and legal consequences.
.png)
Until recently, manufacturer data submission requirements under 340B were largely limited to contract pharmacy claims submitted through the 340B ESP platform. That scope has expanded.
Several manufacturers have updated their policies to require covered entities to submit two additional categories of data in order to maintain access to 340B pricing:
In-house pharmacy claims cover drugs dispensed through entity-owned or operated pharmacies. The data fields required here are the same as those already required for contract pharmacy submissions through ESP, so if you are already submitting contract pharmacy claims, the format is familiar.
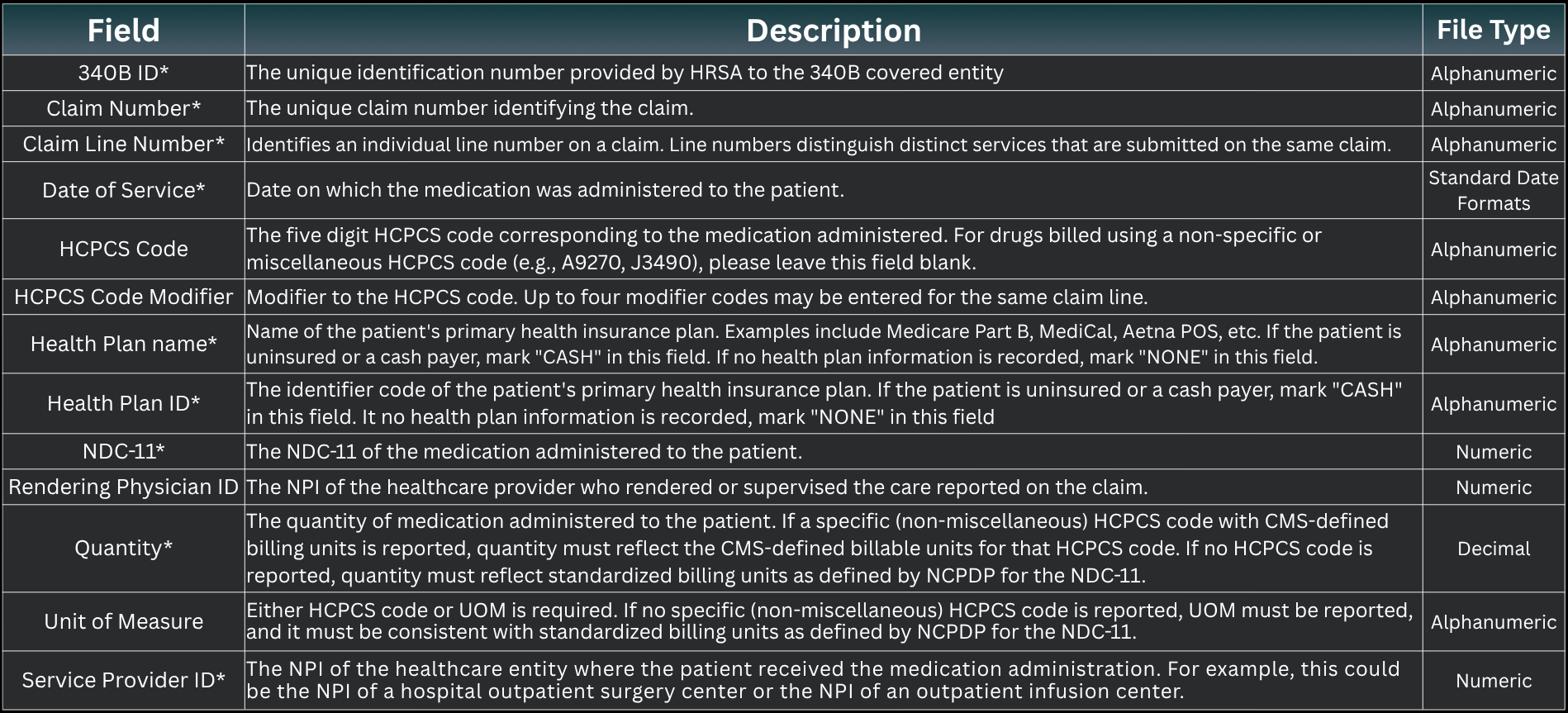
Medical claims cover drugs administered in hospital outpatient or clinic settings. This is a different data specification with additional required fields, including claim number, claim line number, date of service, NDC-11, health plan name and ID, quantity, and service provider NPI. Medical claims data is new territory for most covered entities, and the reporting infrastructure to produce it does not exist out of the box for many organizations.
The manufacturers currently requiring both categories of in-house data are Exelixis, Eli Lilly, Novo Nordisk, AstraZeneca, Bristol Myers Squibb, Biogen, UCB, and Amgen. Their effective dates range from October 2025 through June 2026. State exemptions apply for some manufacturers, so whether a specific policy applies to your entity depends on where you are located.
.png)
One additional development worth watching: Amgen announced that beginning November 15, 2026, it will begin requiring what it describes as standard healthcare visit and service claims data. Amgen would be the first manufacturer to require this type of visit-level data through ESP. The specific data fields have not yet been defined, but Amgen has indicated more detail will be available before the November start date. If other manufacturers follow, this would represent another significant expansion of submission scope.
With Lilly becoming the first manufacturer to terminate 340B pricing access for hospitals that did not comply with its data reporting requirement. The risk is no longer theoretical.
Review your current status with Lilly. If you have not submitted in-house pharmacy claims data, understand what that means for your pricing access and what it would take to come into compliance.
Know where you stand with the other 10 manufacturers that have announced similar requirements. Lilly's action will likely influence how they proceed. Now is a reasonable time to assess your exposure across the board.
Involve your compliance and legal teams. An attorney at the 340B Grantee Conference in late May noted that anything shared in meetings with manufacturers during compliance discussions could be used in subsequent proceedings. Have counsel present for those conversations.
Document everything. Whatever your entity's position, write it down and keep that record current as the situation evolves.
Legal challenges are expected. This will not be resolved through compliance alone, and the outcomes will shape what manufacturers can require going forward.
For many covered entities, the challenge is not the policy decision. It is the data.
Most organizations do not have pre-built reports that generate medical claims in the format manufacturers require. Those reports have to be built, validated, and maintained. Some third-party administrators do not yet have the reporting capabilities to produce the required data, which means entities may need to work directly with their TPA on new data feeds, or generate the data themselves without TPA support.
Covered entities operating alternative distribution models face an additional complication. If you are purchasing drugs through a hospital account and distributing them to a contract pharmacy for dispensing, your purchasing data and your claims data will not align when manufacturers look at both. This mismatch is one reason the new data requirements are putting pressure on ADM strategies.
Document your decision and the reasoning behind it. Whatever your entity decides, write it down, involve compliance and legal teams, and keep that record current as the situation evolves.
Assess your TPA's capabilities. Ask specifically what in-house pharmacy and medical claims reports your TPA can produce today, what gaps exist, and what timeline they have for closing them. Do not assume they are ready.
Lilly recently became the first manufacturer to terminate 340B pricing access for hospitals that did not meet its data reporting requirements, and other manufacturers with similar policies will be watching how it plays out.
Do not meet with manufacturers without legal counsel present. If you receive an outreach requesting a meeting about your submission status, have your legal team involved before you respond and certainly before anyone attends.
RxTrail works with covered entities to evaluate their submission position, understand the operational requirements involved, and develop a strategy for responding to manufacturer data requirements. If you want to talk through where your program stands, reach out.
